
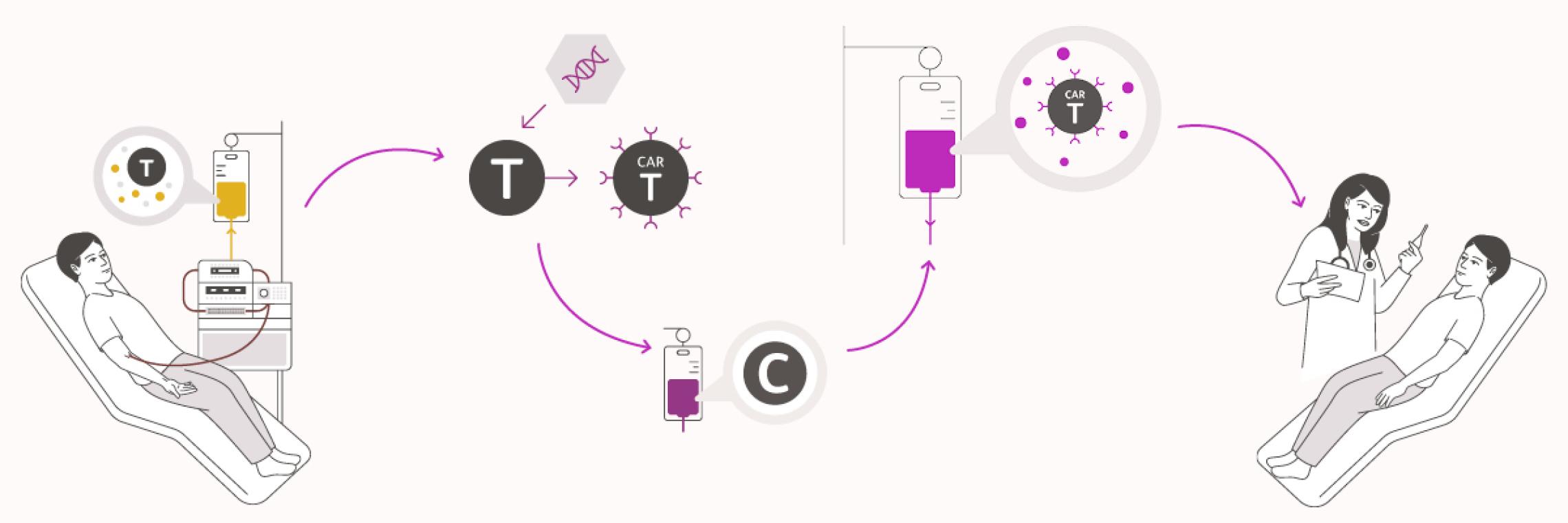
Wie läuft eine CAR-T-Zelltherapie ab?
Eine CAR-T-Zelltherapie besteht aus folgenden Schritten:
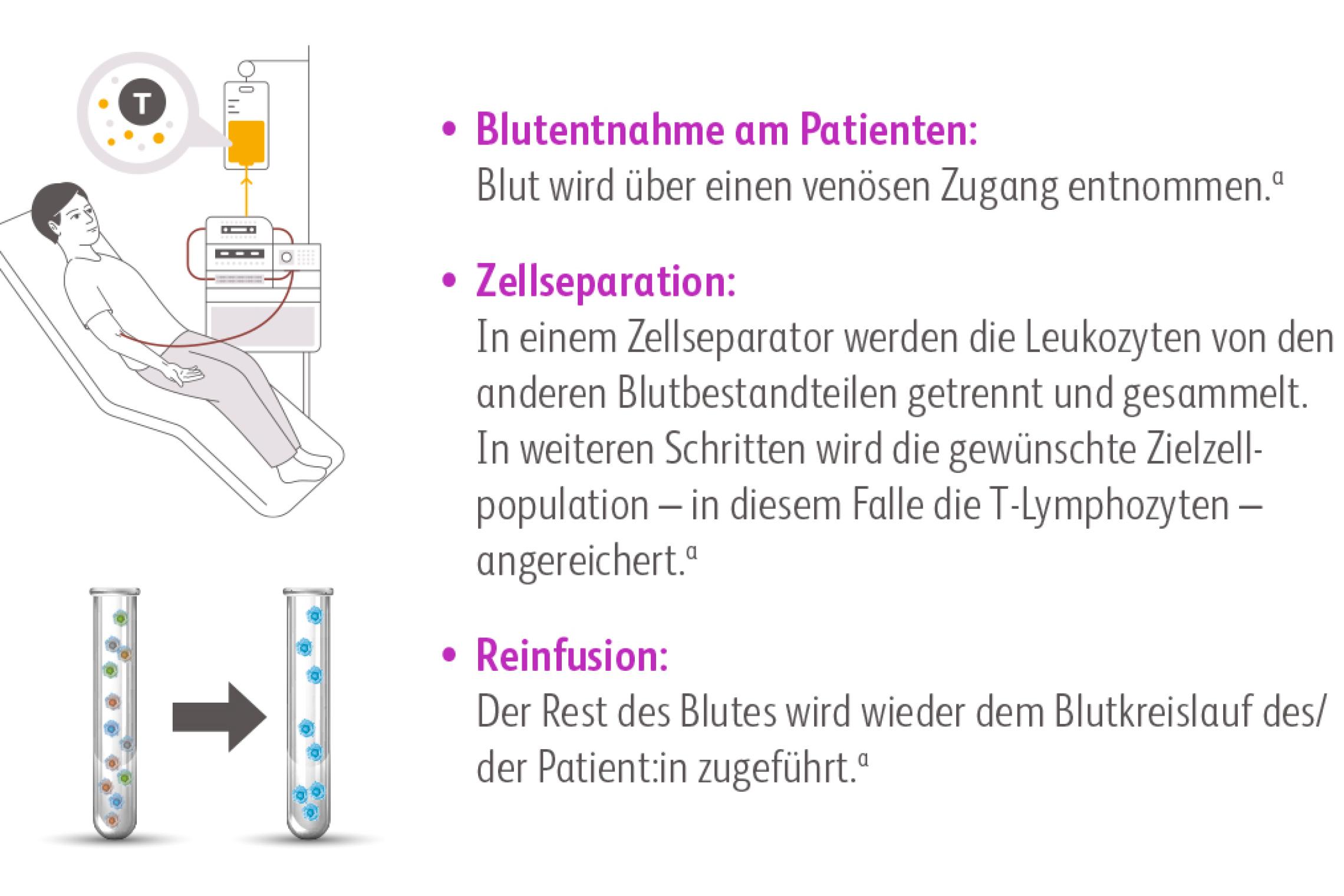
Quelle: a. Levine et al. 2017Levine BL, Miskin J, Wonnacott K, Keir C. Global Manufacturing of CAR T Cell Therapy. Mol Ther Methods Clin Dev. 2017;4:92-101. doi:10.1016/j.omtm.2016.12.006.
Im Gegensatz zur Leukapherese vor einer Stammzelltransplantation müssen die Zellen für die Herstellung von CAR-T Zellen vorher nicht durch Gabe von Wachstumsfaktoren aus dem Knochenmark mobilisiert werden.McGuirk J, Waller EK, Qayed M, et al. Building blocks for institutional preparation of CTL019 delivery. Cytotherapy. 2017;19(9):1015-1024. doi:10.1016/j.jcyt.2017.06.001
Vortherapien können die Anzahl und Qualität von T-Lymphozyten negativ beeinflussen. Daher bedarf es einer engmaschigen Abstimmung der behandelnden Hämatoonkolog:innen mit dem CAR-T-Zentrum, um eine optimale Zellausbeute und Zellqualität bei der Leukapherese zu gewährleisten:McGuirk J, Waller EK, Qayed M, et al. Building blocks for institutional preparation of CTL019 delivery. Cytotherapy. 2017;19(9):1015-1024. doi:10.1016/j.jcyt.2017.06.001 Beaupierre A, Lundberg R, Marrero L, Jain M, Wang T, Alencar MC. Management Across Settings: An Ambulatory and Community Perspective for Patients Undergoing CAR T-Cell Therapy in Multiple Care Settings. Clin J Oncol Nurs. 2019;23(2):27-34. doi:10.1188/19.Cjon.S1.27-34 Yakoub-Agha I, Chabannon C, Bader P, et al. Management of adults and children undergoing chimeric antigen receptor T-cell therapy: best practice recommendations of the European Society for Blood and Marrow Transplantation (EBMT) and the Joint Accreditation Committee of ISCT and EBMT (JACIE). Haematologica. 2020;105(2):297-316. doi:10.3324/haematol.2019.229781
Die CAR-T-Zellen werden für jede/n Patient:in individuell hergestellt. Dieses Verfahren unterliegt intensiven Kontrollen und strengen Qualitätsstandards. Ausführliche Informationen zur Herstellung von CAR-T-Zellen finden Sie auf der Seite CAR-T-Zell-Wissen.
Nach der Leukapherese erfolgt die Herstellung der CAR-T-Zellen. Die Dauer des Herstellungsprozesses kann es notwendig machen, dass die Patient:innen während der Zeit zwischen Leukapherese und CAR-T-Zellinfusion eine Brücken-Antitumortherapie erhalten.Yakoub-Agha I, Chabannon C, Bader P, et al. Management of adults and children undergoing chimeric antigen receptor T-cell therapy: best practice recommendations of the European Society for Blood and Marrow Transplantation (EBMT) and the Joint Accreditation Committee of ISCT and EBMT (JACIE). Haematologica. 2020;105(2):297-316. doi:10.3324/haematol.2019.229781
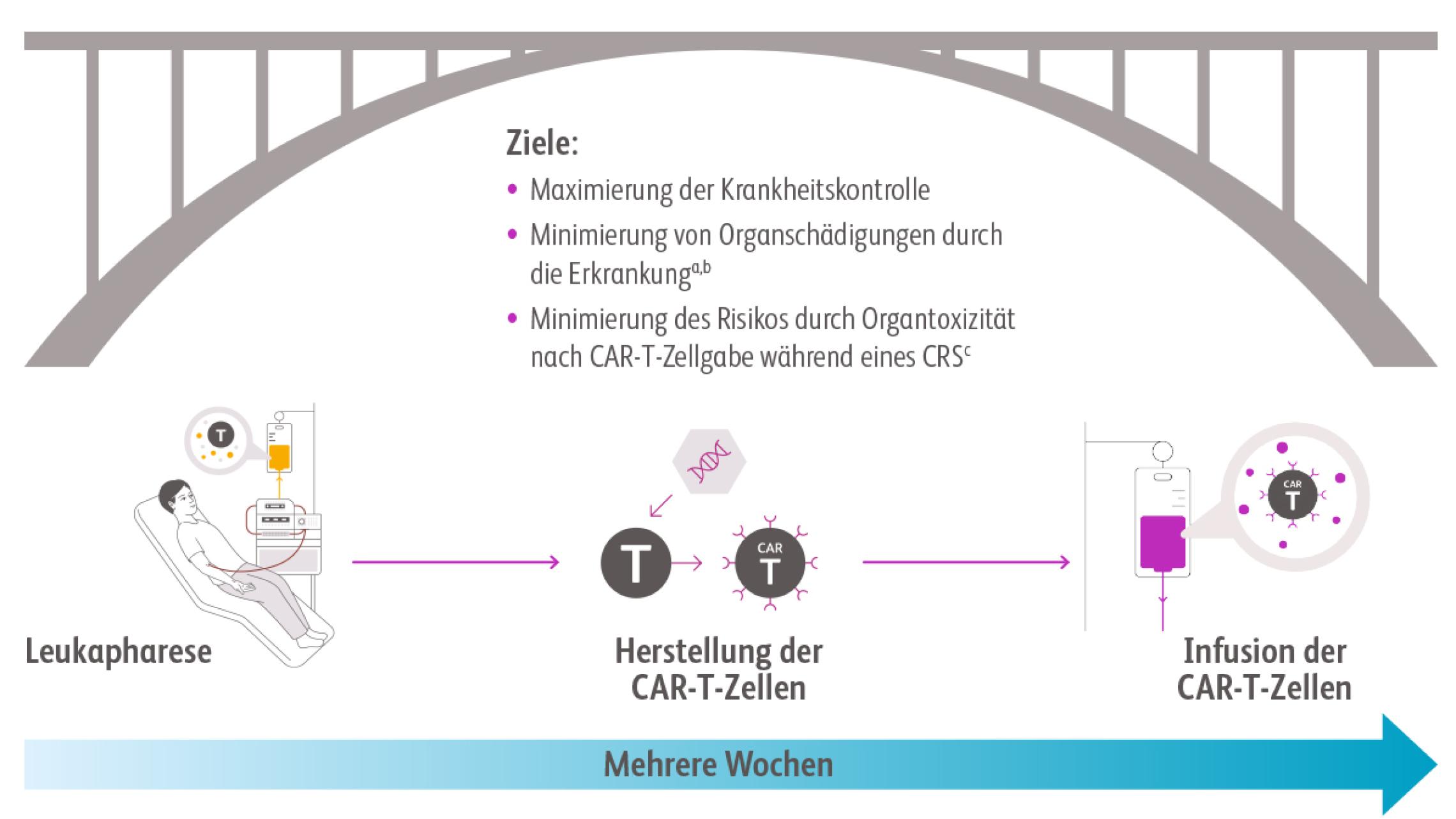
CAR: chimärer Antigenrezeptor, CRS: Zytokinfreisetzungssyndrom; a. McGuirk et al. 2017McGuirk J, Waller EK, Qayed M, et al. Building blocks for institutional preparation of CTL019 delivery. Cytotherapy. 2017;19(9):1015-1024. doi:10.1016/j.jcyt.2017.06.001, b. Yakoub-Agha et al. 2020Yakoub-Agha I, Chabannon C, Bader P, et al. Management of adults and children undergoing chimeric antigen receptor T-cell therapy: best practice recommendations of the European Society for Blood and Marrow Transplantation (EBMT) and the Joint Accreditation Committee of ISCT and EBMT (JACIE). Haematologica. 2020;105(2):297-316. doi:10.3324/haematol.2019.229781, c. Lee et al. 2014Lee DW, Gardner R, Porter DL, et al. Current concepts in the diagnosis and management of cytokine release syndrome. Blood. 2014;124(2):188-95. doi:10.1182/blood-2014-05-552729
Die Brückentherapie kann in Absprache mit dem CAR-T-Zentrum bei den überweisenden Hämatoonkolog:innen erfolgen.
| Die Therapieregime sind variabel und richten sich nach:McGuirk J, Waller EK, Qayed M, et al. Building blocks for institutional preparation of CTL019 delivery. Cytotherapy. 2017;19(9):1015-1024. doi:10.1016/j.jcyt.2017.06.001 Beaupierre A, Lundberg R, Marrero L, Jain M, Wang T, Alencar MC. Management Across Settings: An Ambulatory and Community Perspective for Patients Undergoing CAR T-Cell Therapy in Multiple Care Settings. Clin J Oncol Nurs. 2019;23(2):27-34. doi:10.1188/19.Cjon.S1.27-34 Yakoub-Agha I, Chabannon C, Bader P, et al. Management of adults and children undergoing chimeric antigen receptor T-cell therapy: best practice recommendations of the European Society for Blood and Marrow Transplantation (EBMT) and the Joint Accreditation Committee of ISCT and EBMT (JACIE). Haematologica. 2020;105(2):297-316. doi:10.3324/haematol.2019.229781 |
|---|
|
|
|
|
Bei Patient:innen mit stabiler Erkrankung und geringer Tumorlast ist unter Umständen eine Brückentherapie nicht angezeigt.Yakoub-Agha I, Chabannon C, Bader P, et al. Management of adults and children undergoing chimeric antigen receptor T-cell therapy: best practice recommendations of the European Society for Blood and Marrow Transplantation (EBMT) and the Joint Accreditation Committee of ISCT and EBMT (JACIE). Haematologica. 2020;105(2):297-316. doi:10.3324/haematol.2019.229781
Direkt vor der CAR-T-Zellinfusion erfolgt in der Regel eine Konditionierungsbehandlung (= lymphodepletierende Chemotherapie (LDC)) in Form einer milden Chemotherapie. Diese soll die Anzahl der Immunzellen und vorhandenen Tumorzellen im Körper des/der Patient:in reduzieren und so ein günstiges Milieu für die Vermehrung der CAR-T-Zellen schaffen.Yakoub-Agha I, Chabannon C, Bader P, et al. Management of adults and children undergoing chimeric antigen receptor T-cell therapy: best practice recommendations of the European Society for Blood and Marrow Transplantation (EBMT) and the Joint Accreditation Committee of ISCT and EBMT (JACIE). Haematologica. 2020;105(2):297-316. doi:10.3324/haematol.2019.229781
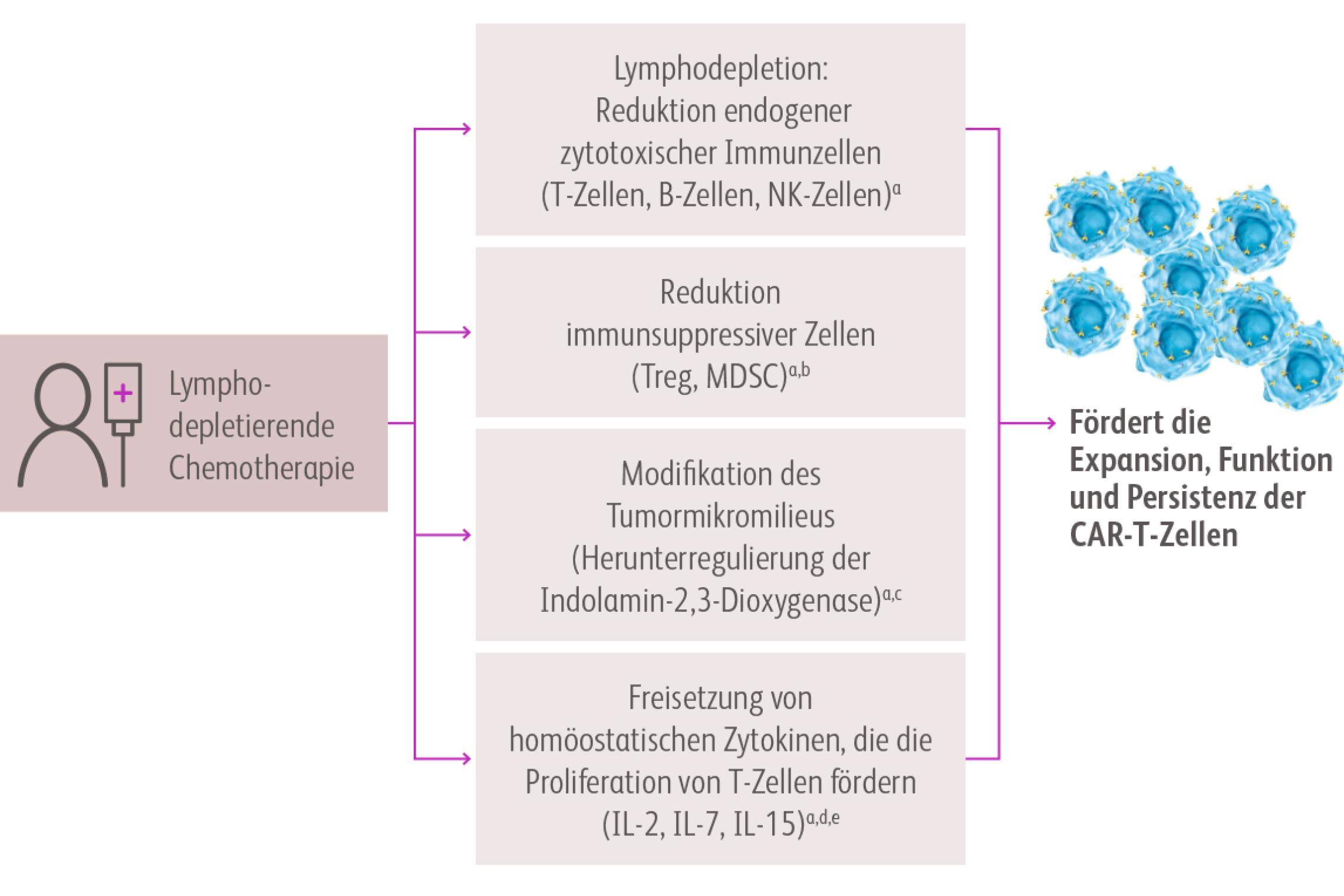
CAR: chimärer Antigenrezeptor, IL: Interleukin, MDSC: myeloide Suppressorzelle, NK: natürliche Killerzelle, Treg: regulatorische T-Zelle. Quellen: a. Neelapu et al. 2019Neelapu SS. CAR-T efficacy: is conditioning the key? Blood. 2019;133(17):1799-1800. doi:10.1182/blood-2019-03-90092, b. Lee et al. 2011, c. Gattinoni et al. 2005, d. Hirayama et al. 2019.
Häufig wird für die Lymphodepletion eine Kombination aus Fludarabin und Cyclophosphamid eingesetzt, die in niedriger Dosierung für ca. 3 Tage direkt vor der CAR-T-Zellinfusion (mindestens 2 Tage Pause dazwischen) verabreicht werden.Yakoub-Agha I, Chabannon C, Bader P, et al. Management of adults and children undergoing chimeric antigen receptor T-cell therapy: best practice recommendations of the European Society for Blood and Marrow Transplantation (EBMT) and the Joint Accreditation Committee of ISCT and EBMT (JACIE). Haematologica. 2020;105(2):297-316. doi:10.3324/haematol.2019.229781 Brudno JN, Kochenderfer JN. Recent advances in CAR T-cell toxicity: Mechanisms, manifestations and management. Blood Rev. 2019;34:45-55. doi:10.1016/j.blre.2018.11.002 Perica K, Curran KJ, Brentjens RJ, Giralt SA. Building a CAR Garage: Preparing for the Delivery of Commercial CAR T Cell Products at Memorial Sloan Kettering Cancer Center. Biol Blood Marrow Transplant. 2018;24(6):1135-1141. doi:10.1016/j.bbmt.2018.02.018 Hayden PJ, Roddie C, Bader P, et al. Management of adults and children receiving CAR T-cell therapy: 2021 best practice recommendations of the European Society for Blood and Marrow Transplantation (EBMT) and the Joint Accreditation Committee of ISCT and EBMT (JACIE) and the European Haematology Association (EHA). Ann Oncol. 2022;33(3):259-275. doi:10.1016/j.annonc.2021.12.003
Die Art der lymphodepletierenden Chemotherapie ist in der produktspezifischen Fachinformation angegeben.
Während der Infusion wird der/die Patient:in streng überwacht, um im Falle von unerwünschten Reaktionen sofort reagieren zu können.Yakoub-Agha I, Chabannon C, Bader P, et al. Management of adults and children undergoing chimeric antigen receptor T-cell therapy: best practice recommendations of the European Society for Blood and Marrow Transplantation (EBMT) and the Joint Accreditation Committee of ISCT and EBMT (JACIE). Haematologica. 2020;105(2):297-316. doi:10.3324/haematol.2019.229781 Hayden PJ, Roddie C, Bader P, et al. Management of adults and children receiving CAR T-cell therapy: 2021 best practice recommendations of the European Society for Blood and Marrow Transplantation (EBMT) and the Joint Accreditation Committee of ISCT and EBMT (JACIE) and the European Haematology Association (EHA). Ann Oncol. 2022;33(3):259-275. doi:10.1016/j.annonc.2021.12.003
| Gründe für eine verzögerte Anwendung |
|---|
Die Infusion der CAR-T-Zellen muss unter bestimmten Umständen aufgeschoben werden. Gründe für eine verzögerte Anwendung können beispielsweise sein:Yakoub-Agha I, Chabannon C, Bader P, et al. Management of adults and children undergoing chimeric antigen receptor T-cell therapy: best practice recommendations of the European Society for Blood and Marrow Transplantation (EBMT) and the Joint Accreditation Committee of ISCT and EBMT (JACIE). Haematologica. 2020;105(2):297-316. doi:10.3324/haematol.2019.229781 |
|
|